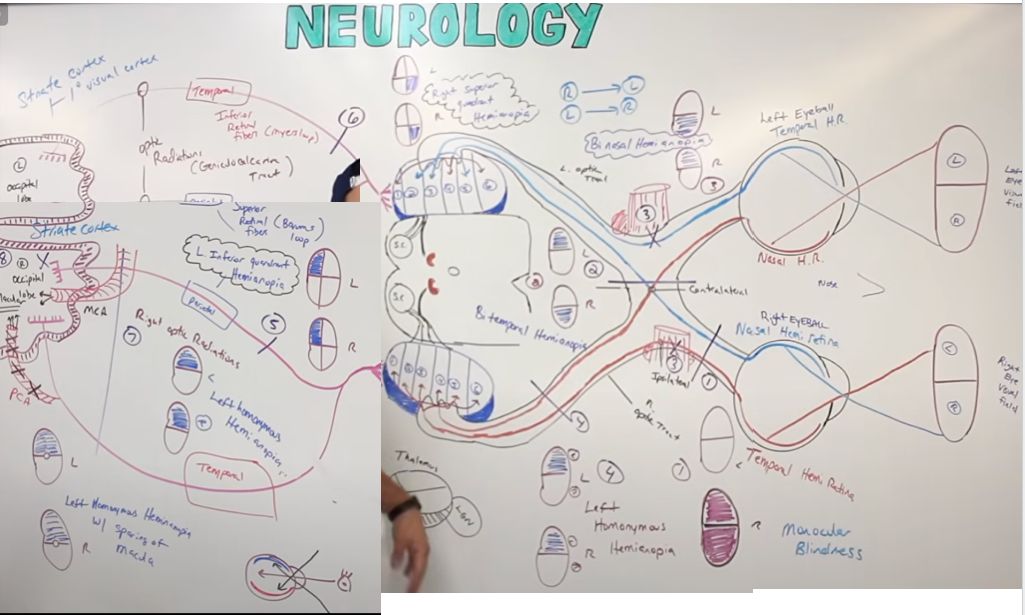
CN II Optic :: Visual Pathway
Light from the left[…] visual field hits the right[…] hemiretina of each eye.
From the right eye, fibers travel via optic nerve → do not cross[…] the optic chiasm → right optic tract. From the left eye, fibers travel via optic nerve → cross[…] the optic chiasm → right optic tract.
Both tracts synapse at the lateral geniculate nucleus (LGN)[…] of the thalamus: ipsilateral fibers go to layers 2, 3, 5[…]; contralateral fibers go to layers 1, 4, 6[…].
Some LGN fibers project to the superior colliculus and pretectal nucleus[…] in the midbrain (for the light reflex and saccades).
The rest project as the optic radiations through the parietal lobe (Baum's loop, superior fibers)[…] and temporal lobe (Meyer's loop, inferior fibers)[…], arriving at the primary visual cortex (V1)[…] along the calcarine sulcus.