HIBI - Pathophysiology
Subclassification: pediatric, in-hospital (IHCA, higher ROSC), and out-of-hospital (OHCA, lower survival). "Two-Hit" Model: Primary[…] brain injury from ischemia during pulselessness → made worse by reperfusion[…] injury via ROS and inflammation.
Impaired aerobic metabolism → loss of ATP → anoxic depolarization → cytotoxic edema[…].
Increased anaerobic metabolism → lactate accumulation → intracellular acidosis → increased intracellular Ca+2 → mitochondrial toxicity[…].
Disproportionately hits metabolically active structures: cortex, hippocampus, basal ganglia, thalami, cerebellar vermis[…].
Secondary[…] brain injury: neuroinflammation from imbalance between O2 delivery and metabolic demand.
Triggers: fever, seizures[…], cerebral edema, and disrupted autoregulation.
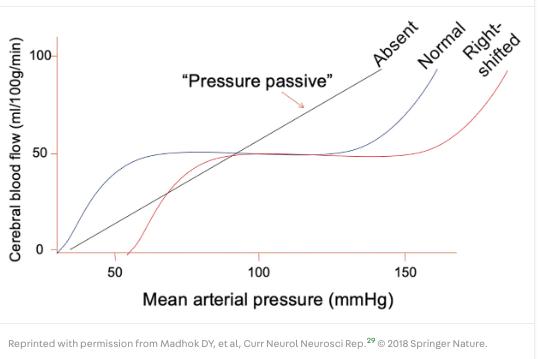
The lower limit of cerebral autoregulation shifts right[…] or is absent → CPP insufficient even at normal MAP.