Migraine - Pathophysiology
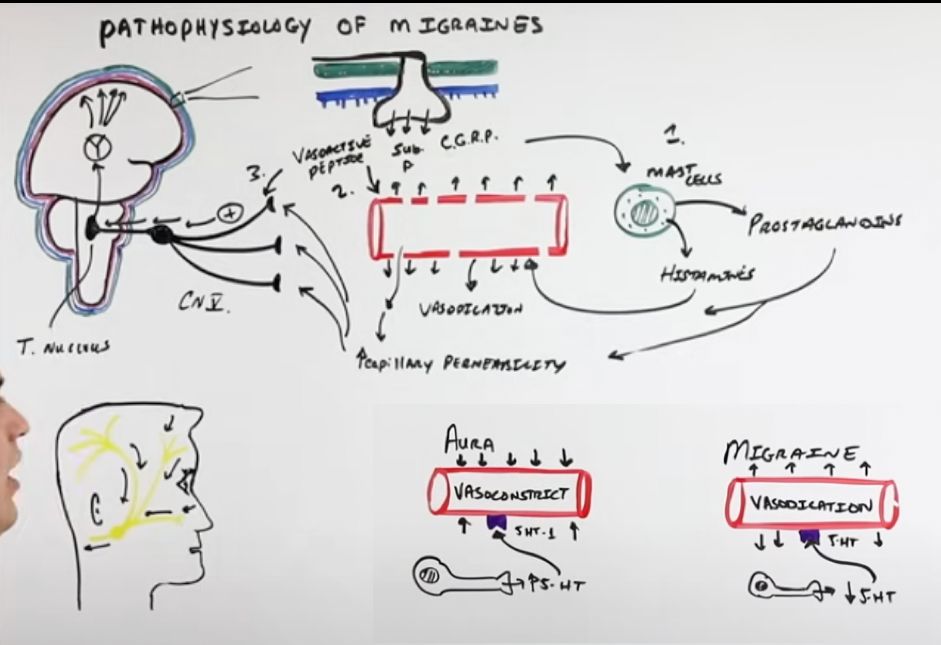
HA pathophysiology: First: irritation of nociceptors connected to CN V[…] supplying the dura mater[…] → release NTs: vasoactive peptide, substance P, and CGRP[…]; They act on mast cells[…] to release histamine + prostaglandins[…] → vasodilate BVs + increase capillary permeability; They also act directly on BVs to release NO[…] → similar response; Inflammatory mediators activate nearby nociceptors → action potentials down CN V → trigeminal ganglion → trigeminal nucleus → thalamus → primary somatosensory cortex.
Pathophysiology of aura: Effects above increase release of K+ and glutamate[…] from neurons faster than glial cells can clear → triggers Cortical Spreading Depression[…] (sustained propagating depolarization, self-regenerating positive feedback loop) → burns itself out (explains visual aura → temporary scotoma); High serotonin[…] often seen in aura → acts on 5-HT receptors → vasoconstricts BVs; Low serotonin[…] → associated with vasodilation and migraine without aura.