EEG - Basic Neurophysiology
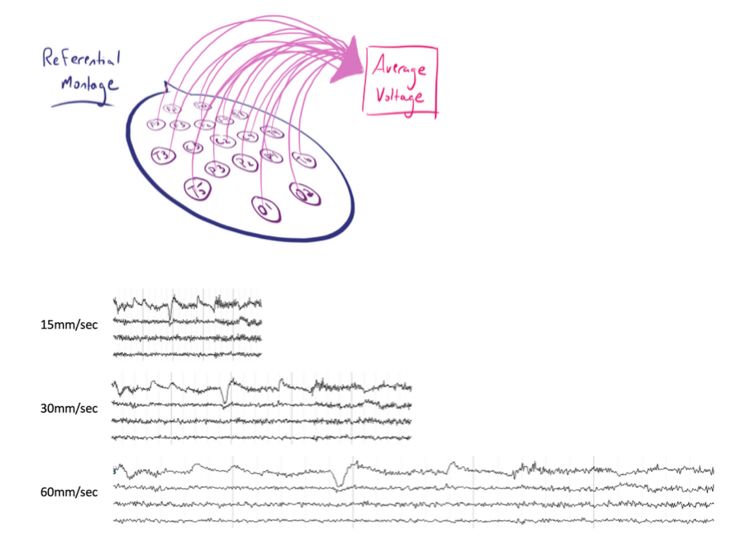
- we need >6[…]cm2 of synchronized cortical activity for anything to be detected on scalp EEG
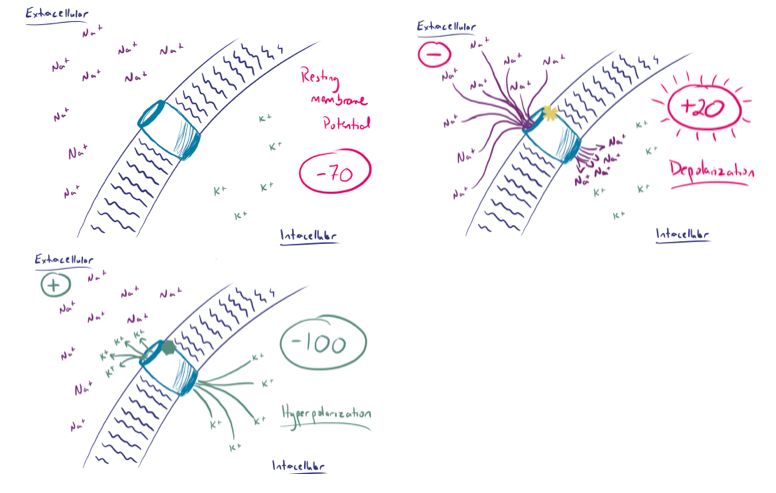
- the resting potential inside the cell is -70[…]mV established by Na/K ATPase[…] channel
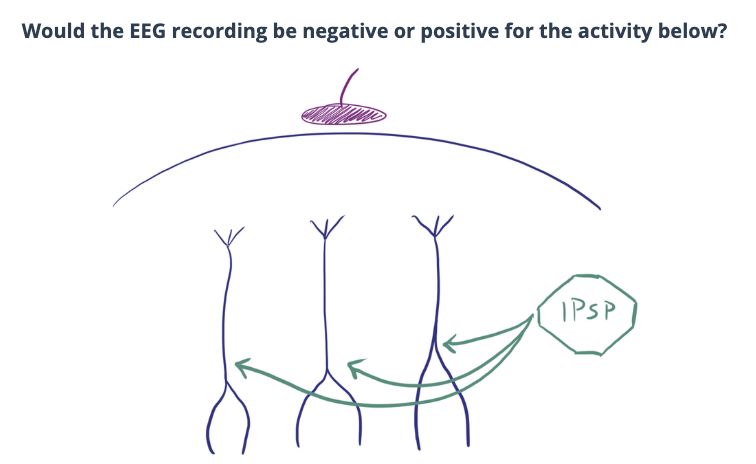
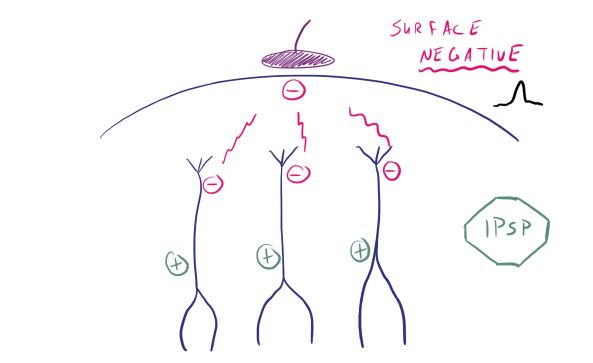
- depolarization leads to Na+ rushing into the cell making the resting potential less[…](-) (aka more[…]+) while the extracellular area becomes more (-)[…]
- hyperpolarization leads to K- rushing out of the cell making the resting potential more[…](-) (aka less[…]+) while the extracellular area becomes more (+)[…]
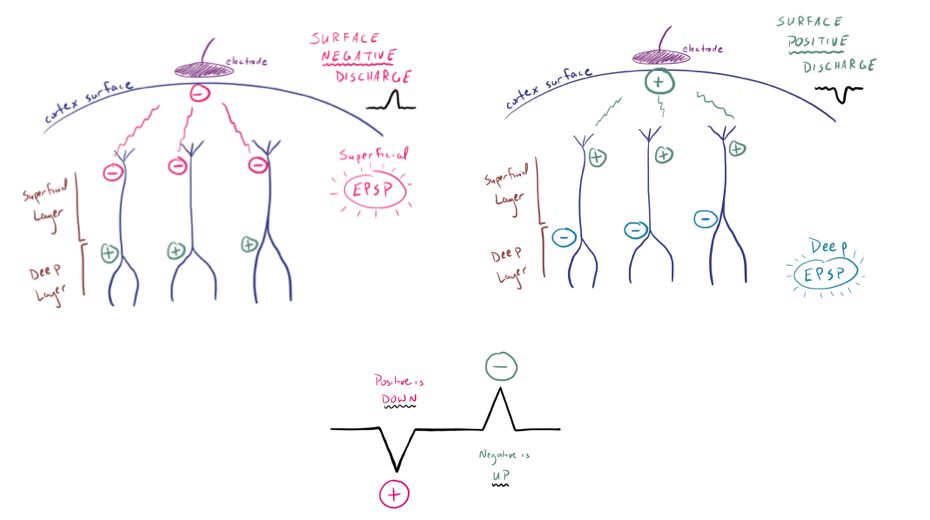
- Excitatory neurotransmitters such as glutamate[…] bind to postsynaptic receptors and cause an excitatory postsynaptic potential (EPSP)[…]
- Inhibitory neurotransmitters, such as GABA[…], cause an inhibitory postsynaptic potential (IPSP[…])