Cognitive Symptoms - Clinical Approach
Clarify the presenting symptom: "Memory loss" for words → actually aphasia[…]; "Memory loss" for every day actions → actually working memory/attention[…] impairment; "Memory loss" for faces → actually prosopagnosia[…].
Functional capacity: preserved in MCI[…]; progressively impaired in dementia[…].
Cognitive domains: Attention[…]: assessed first; needed for all other domains; tested with forward digit span, backward digit span, serial 7s, Trail Making[…] test, letter cancellation.
Language[…]: articulation, fluency, prosody, grammar/syntax.
Phonemic paraphasias = wrong phoneme ("gaise" for "raise"); semantic paraphasias[…] = wrong word ("orange" for "apple"); agrammatism = telegraphic speech; aprosodia = loss of melodic tone (nondominant hemisphere).
Memory[…]: focus on explicit/declarative.
Retrograde = old events; anterograde = can't form new (localizes to hippocampus[…]).
True amnesia = no free or cued recall; retrieval disorder = cued recall preserved (localizes to frontal/subcortical[…] region).
Visuospatial[…]: apperceptive agnosia (can't copy figure) vs associative agnosia (can't access stored knowledge — prosopagnosia, pure alexia, achromatopsia, visual object agnosia[…]).
Executive[…]: multitasking tests.
Cognitive impairment phenotypes by localization: Amnestic → limbic system[…]; Language → dominant hemisphere; Visuospatial → parietooccipital or temporooccipital; Dysexecutive → prefrontal cortex or subcortical connections[…] (BG > thalamus, cerebellar).
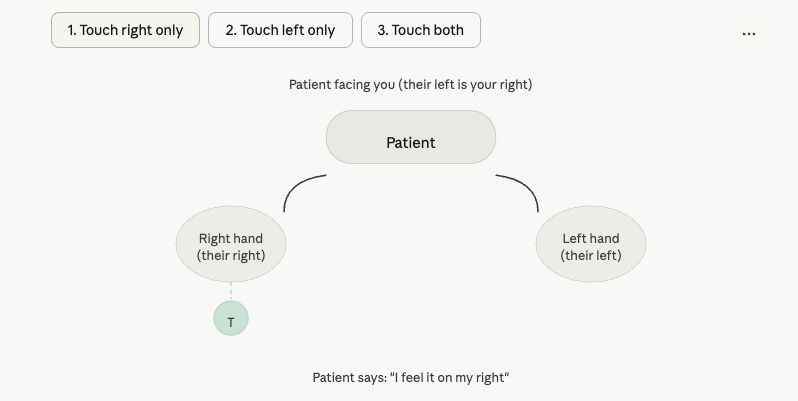
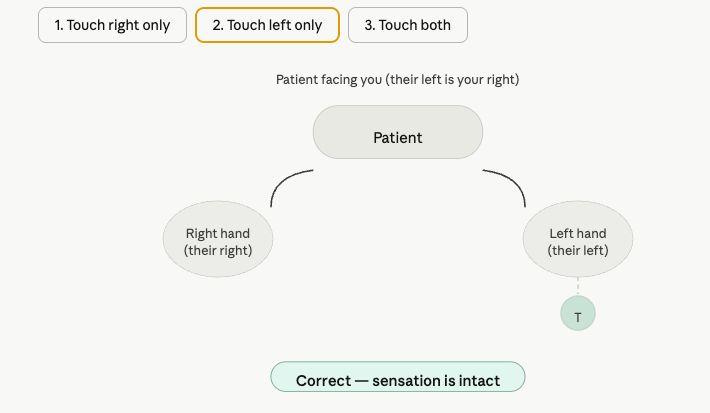
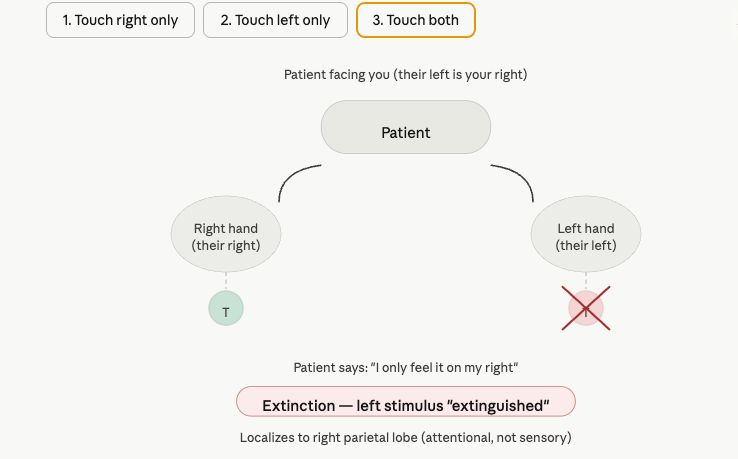
Exam findings: Paratonia (can't relax) → frontal-subcortical dysfunction; Frontal release signs (grasp/snout/glabellar/palmomental): little diagnostic value, can be seen in healthy adults; Cortical sensory loss: tested with graphesthesia, stereognosis, extinction[…]. Diagnostics: serum CMP + B12 + TSH ± HIV/syphilis; MRI brain ± LP if infectious/autoimmune; EEG if prion suspected, fluctuating symptoms, or seizures concern.