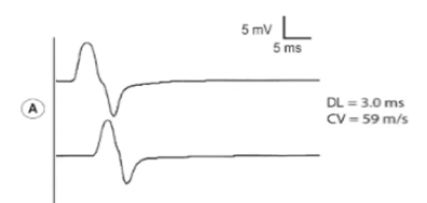
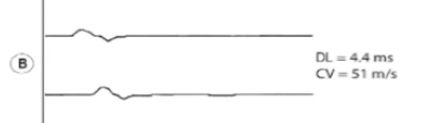
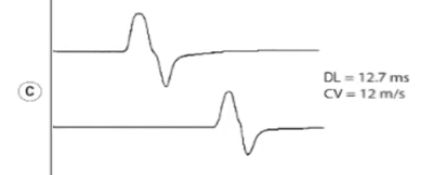
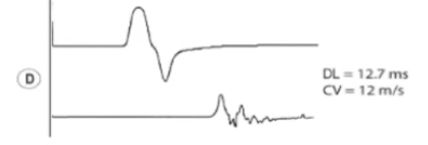
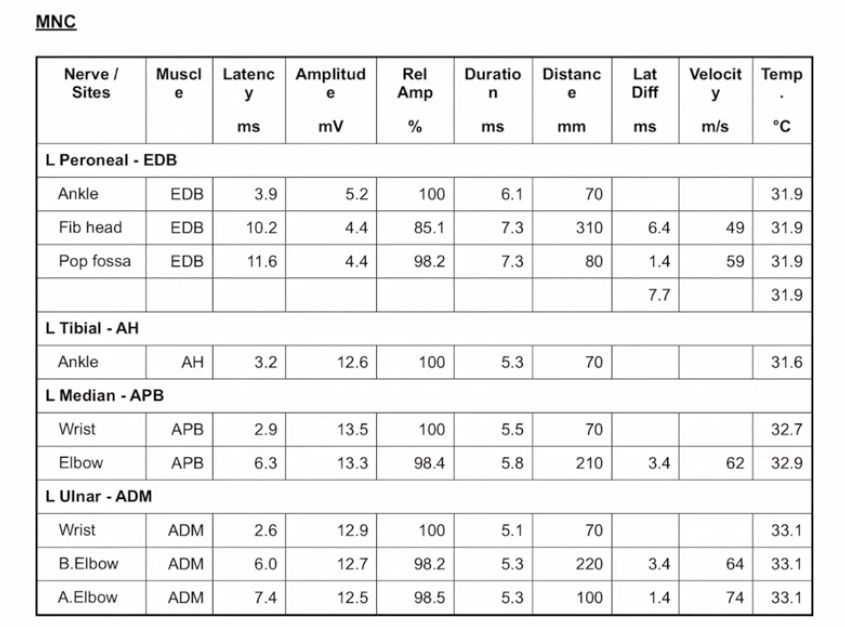
In AIDP, increased CMAP duration is due to temporal dispersion[…] from nerves losing their insulation, so signals arrive at muscles at different times and the electrical signal gets stretched out. Low temperature[…] just slows everything but doesn’t cause temporal dispersion[…].
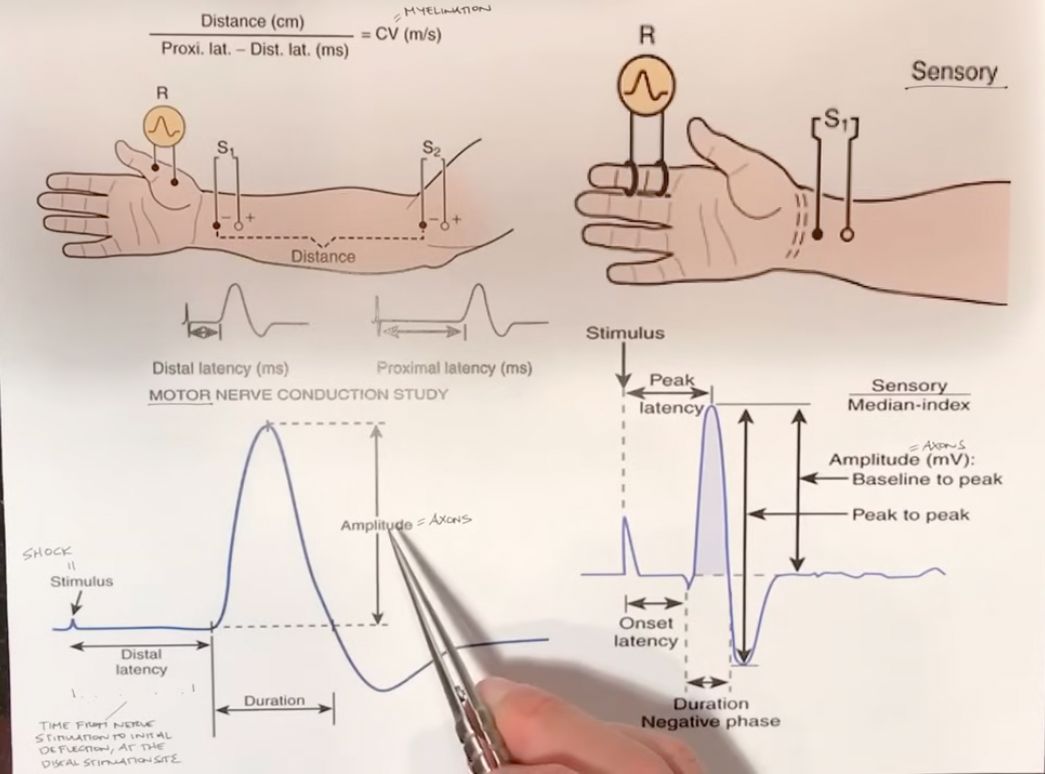
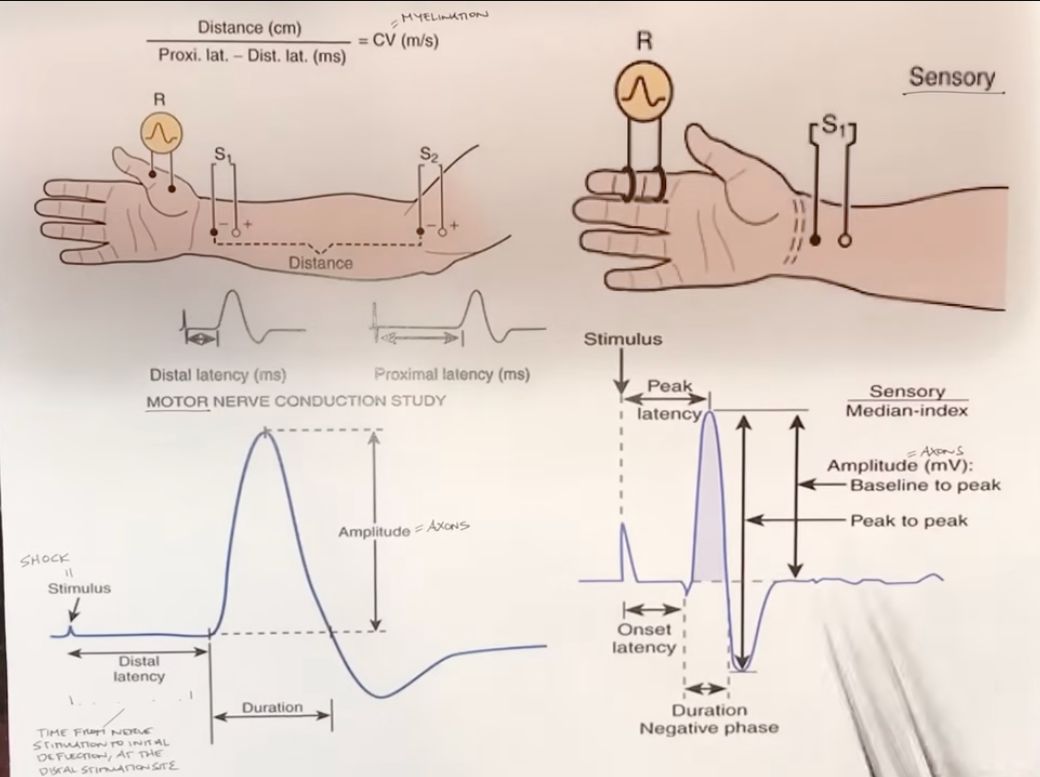
- A CMAP[…] is the electrical sum of many muscle fibers summed up
- Delay at the NMJ[…] affects onset latency[…], not duration (delays start time for the signal)