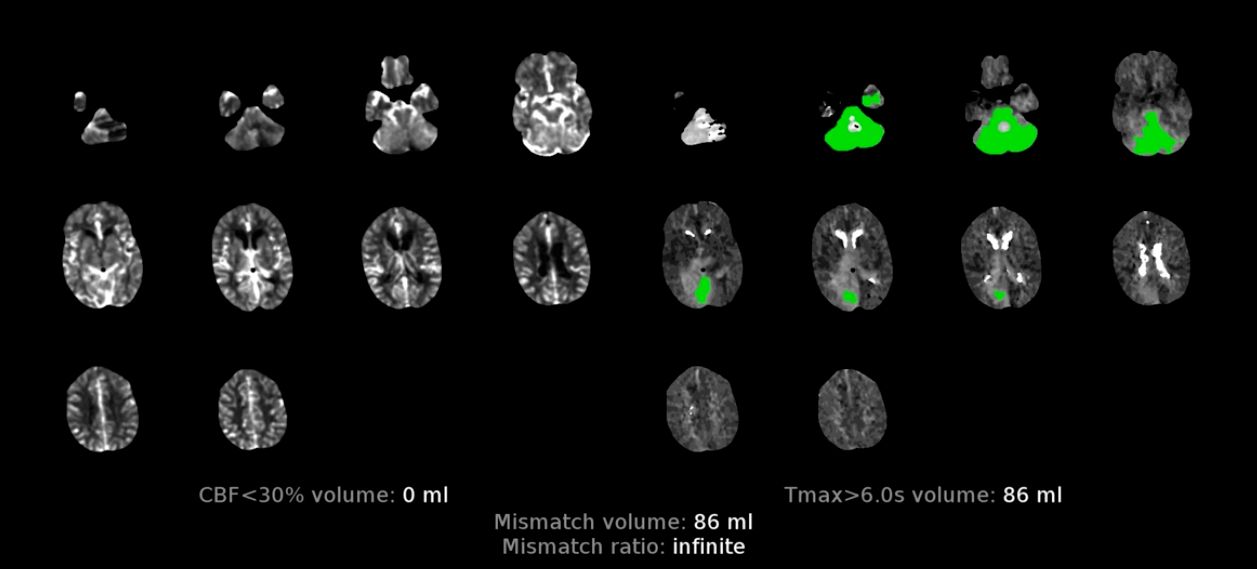
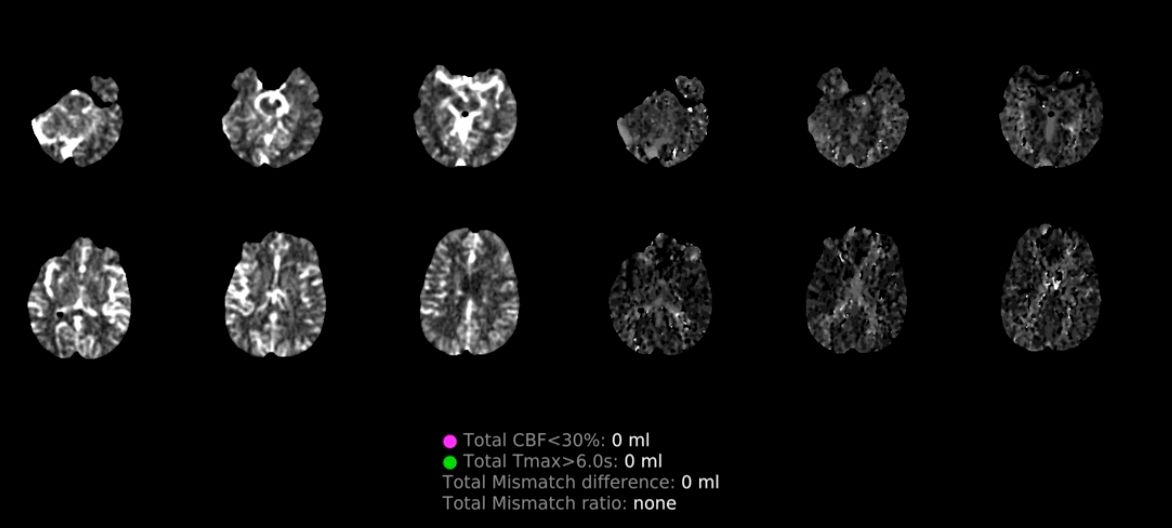
CTP Basics
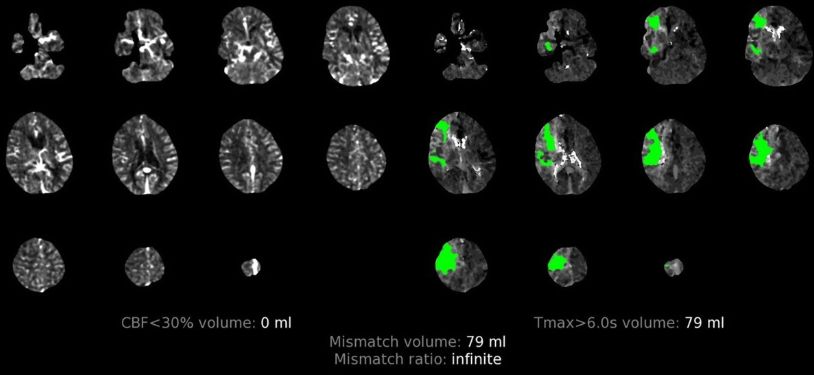
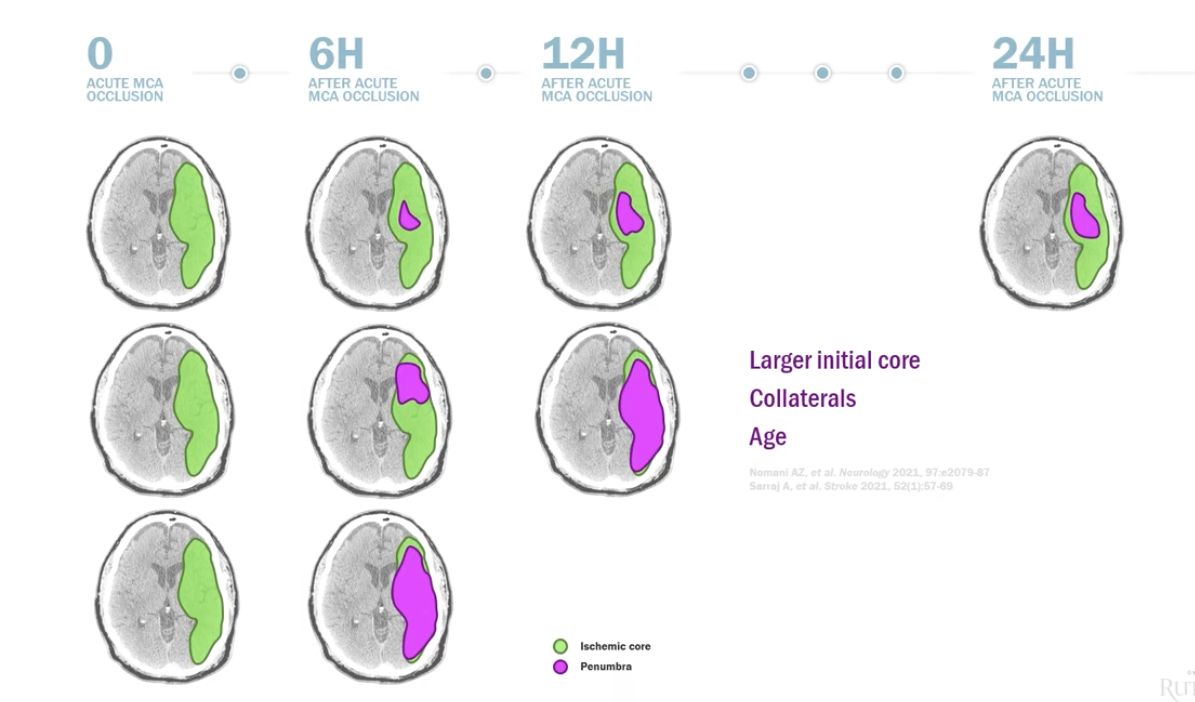
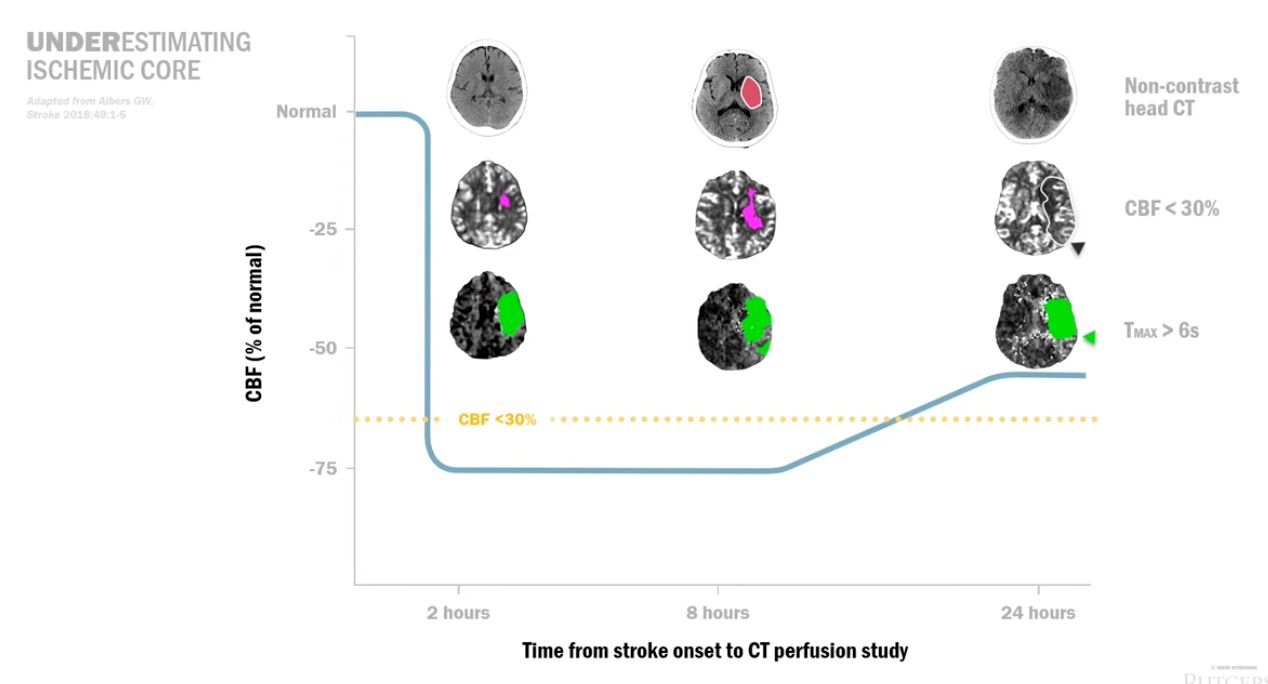
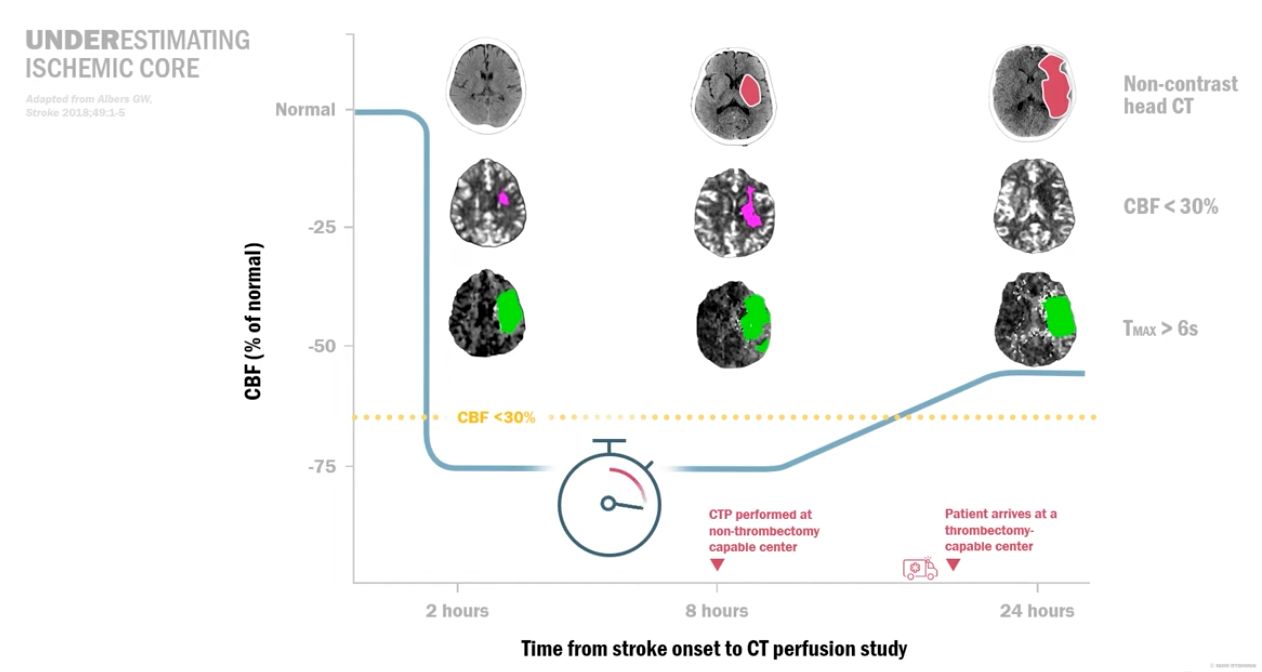
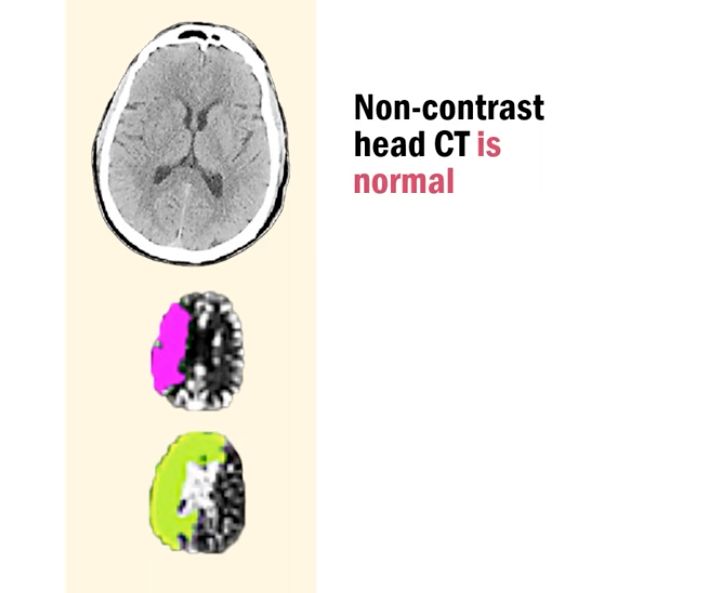
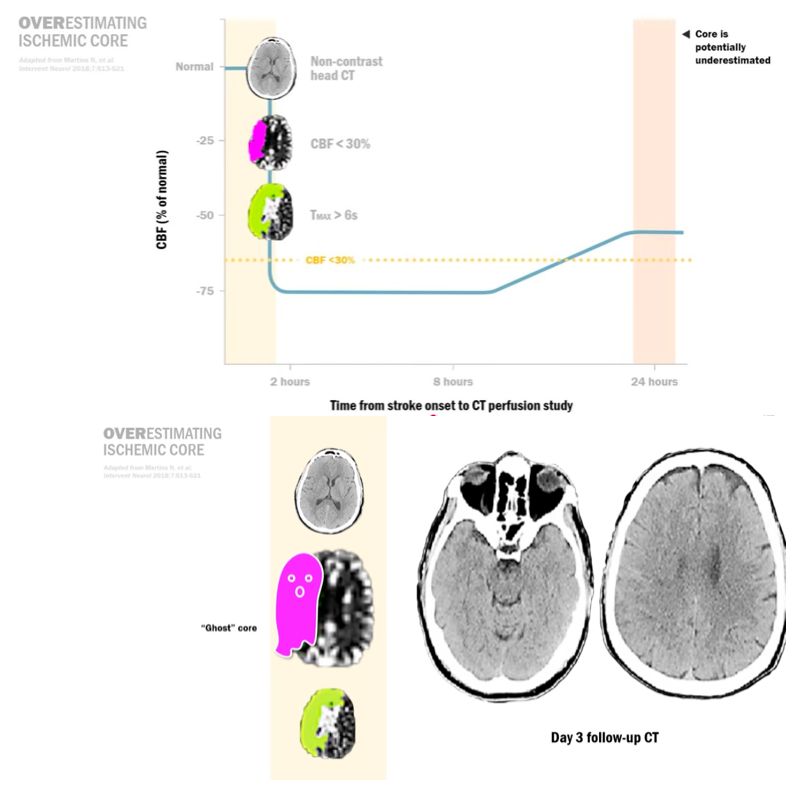
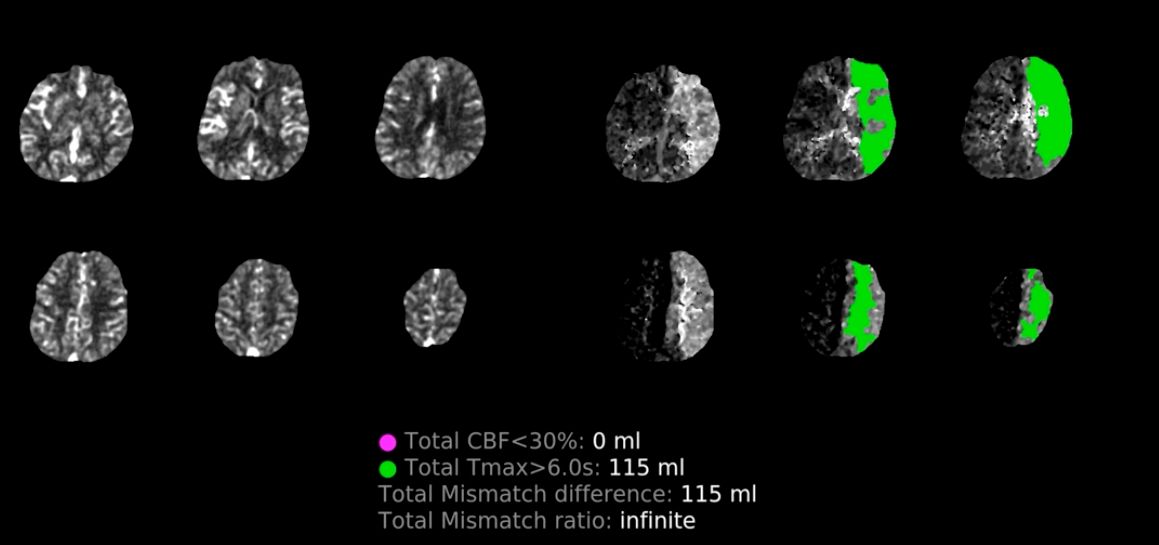
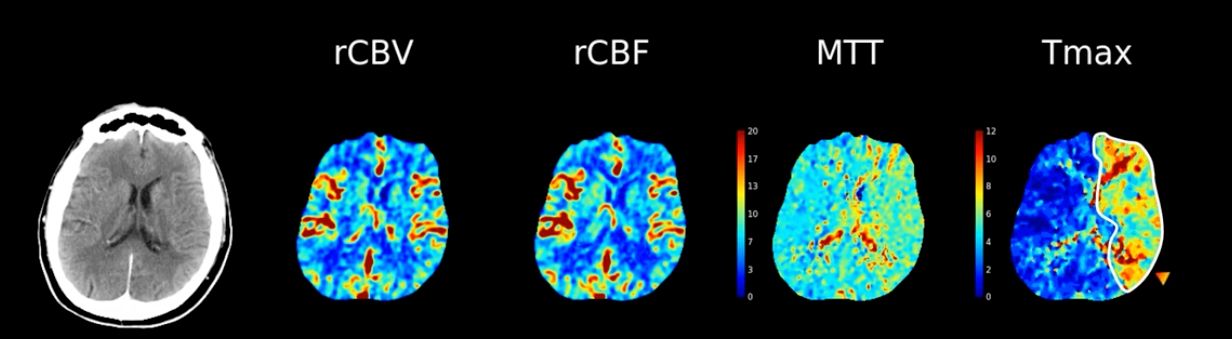
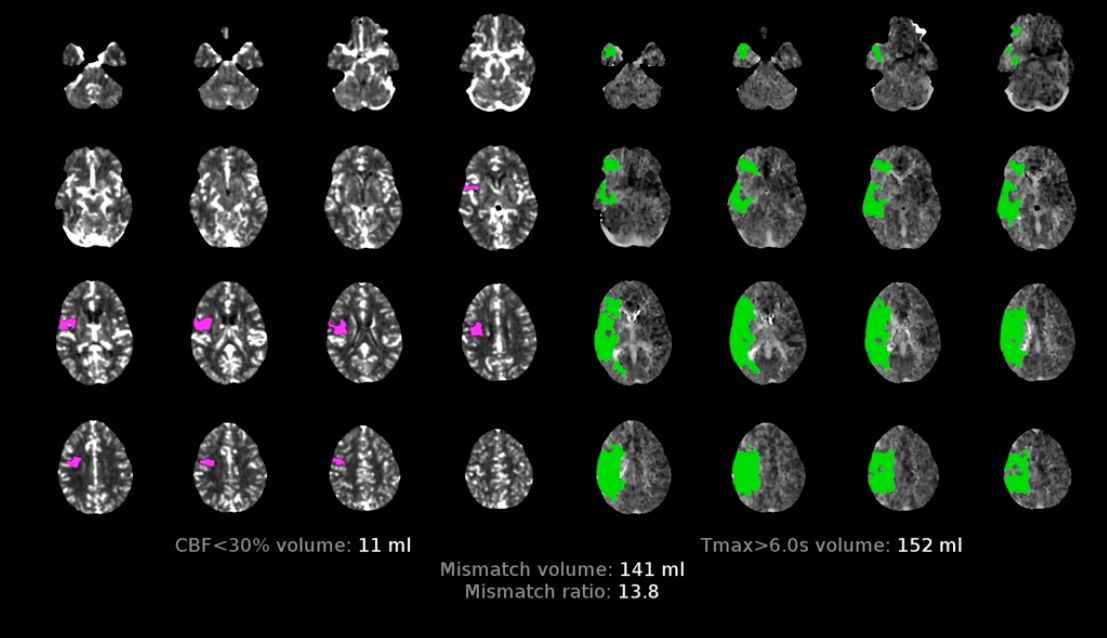
- CBF<30[…]%: this is defined as the volume of brain tissue with calculated CBF[…] less than 30[…]% compared to the contralateral[…] hemisphere, purple[…] color, corresponding to infarct core[…] = area of irreversible[…] tissue damage
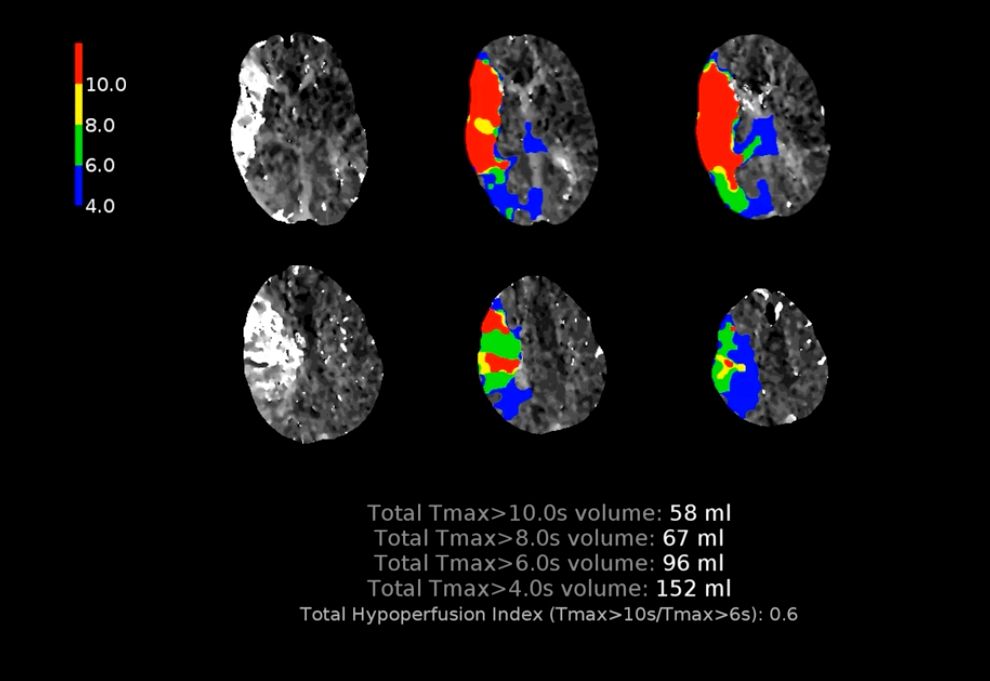
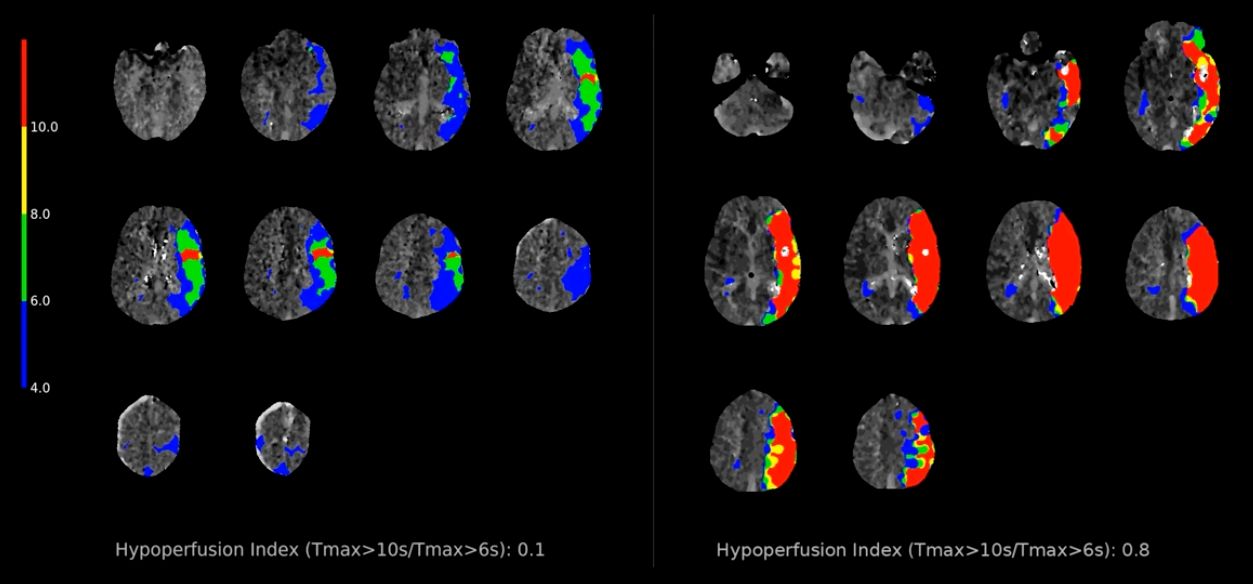
- Tmax>6[…]s: this is defined as the volume of brain tissue with greater than 6[…]s delay in the arrival of dye bolus, green[…] color, corresponding to the infarct penumbra[…] = area of reversible[…] tissue damage