Childhood and Adolescent Epilepsy Syndromes
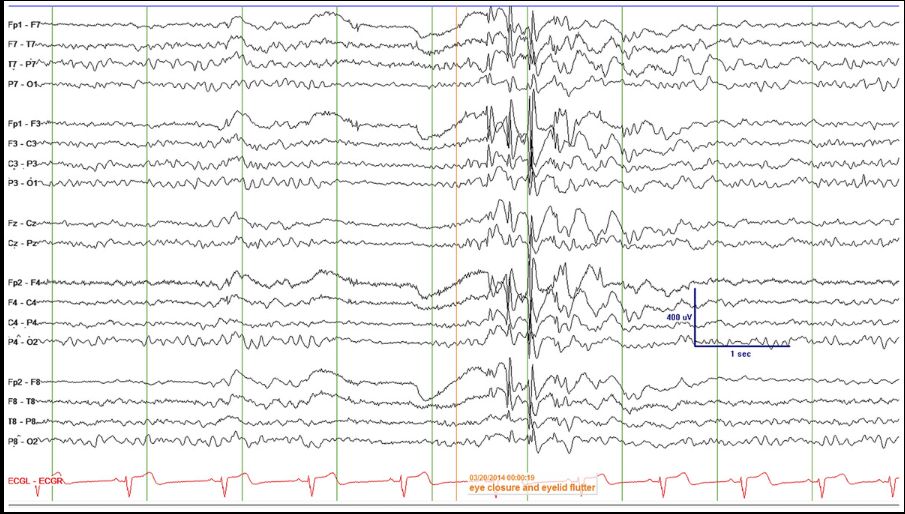
Late-onset childhood occipital epilepsy (Gastaut type): peak 8-11 yo. Visual hallucinations + ocular pain + transient vision loss → postictal HA. EEG: bilateral occipital spike-and-wave activated by eye closure, attenuated by eye opening (fixation off phenomenon)[…].
Childhood Absence Epilepsy (Pyknolepsy): 4-10 yo, peak 5-7 yo.: Onset <4 yo: consider GLUT1 deficiency[…].
Pathophys: CACNA1A, GABRG2, GABRG3[…] mutations → cortico-thalamic dysfunction; nucleus reticularis thalamus oscillates via T-type Ca+2 channels. Typical absence: behavioral arrest/staring + automatisms.
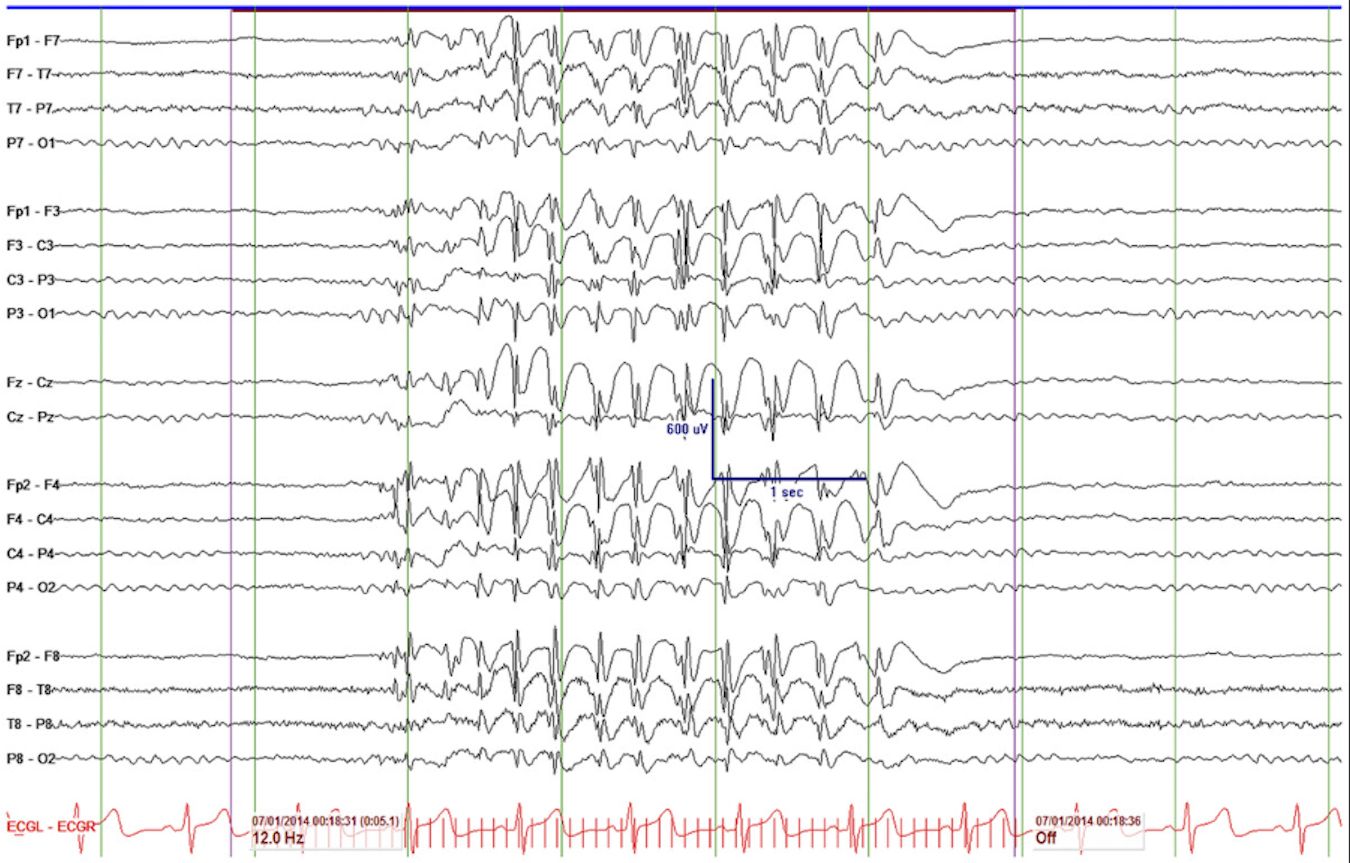
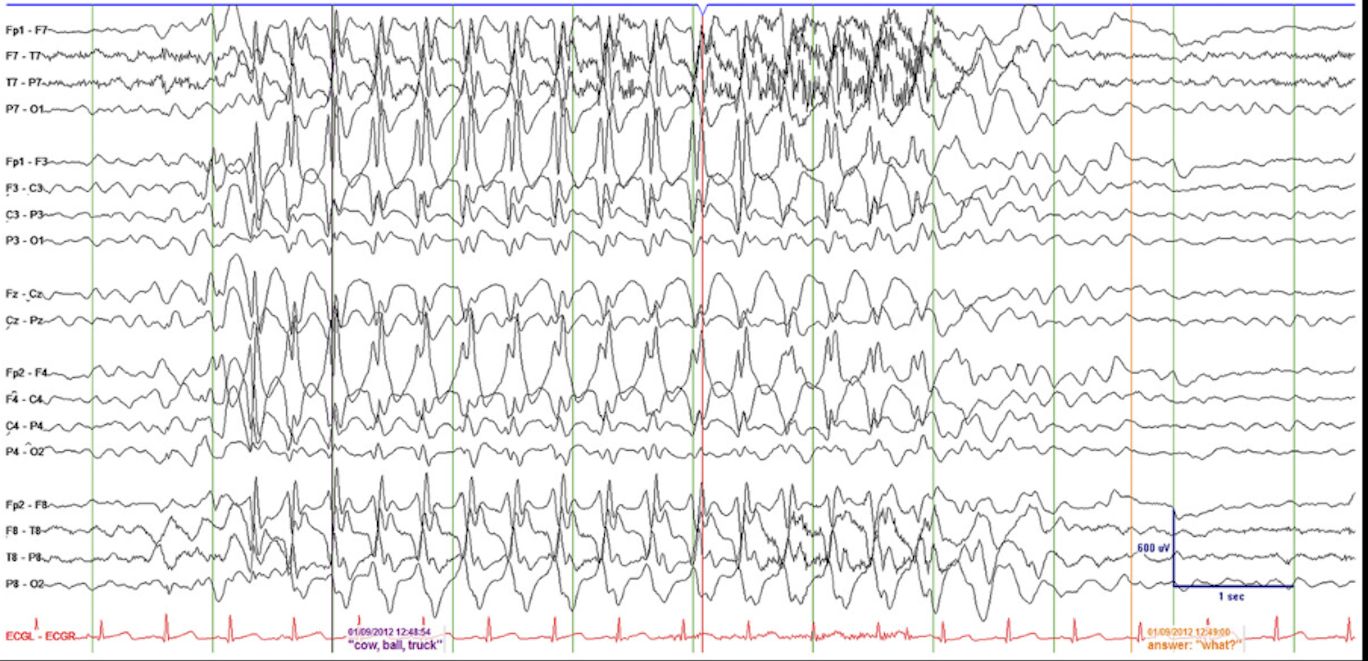
EEG: generalized bilateral synchronous 3-4 Hz[…] spike-and-wave, frontal dominant; abrupt onset/offset.
Hyperventilation[…] activates.
Treatment: T-type Ca+2 blockers — ethosuximide[…] first-line, or VPA.
GABAb agonists (vigabatrin)[…] can worsen. JAE (Juvenile Absence Epilepsy): peak 15 yo. Absence seizures more sporadic and longer than CAE. EEG: 3-4 Hz spike/polyspike. Treatment: ethosuximide for absence + VPA or lamotrigine.
Avoid phenytoin, carbamazepine, gabapentin/pregabalin, vigabatrin[…].
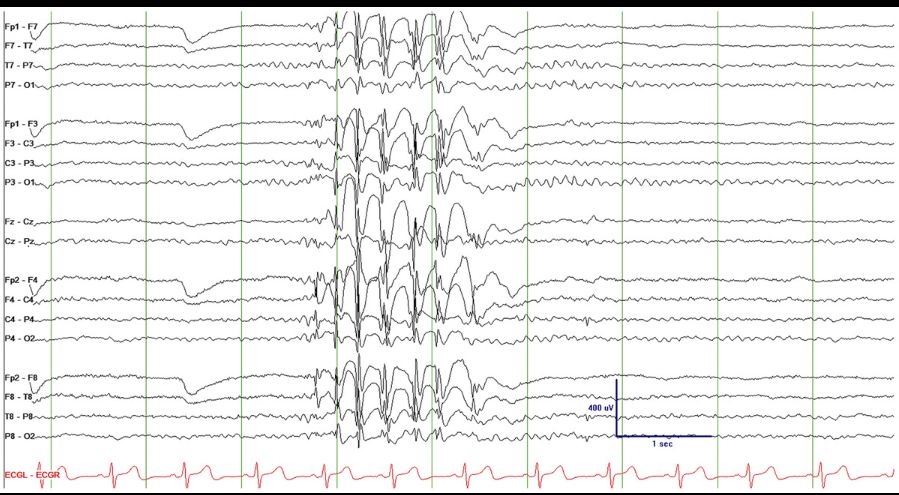
JME (Juvenile Myoclonic Epilepsy): most constant feature is myoclonic seizures upper extremities on awakening[…] → majority develop GTC + absence.
EEG: 4-6 Hz[…] generalized spike/polyspike-and-slow-wave (inverted W) potentiated by sleep deprivation. Treatment: VPA (avoid in women of childbearing age) or keppra/lamotrigine. Avoid same drugs as JAE. Mesial temporal lobe epilepsy with hippocampal sclerosis: Childhood-adolescence; associated with prior febrile SE. Pathology: atrophy + gliosis of hippocampus, amygdala, parahippocampal gyrus, entorhinal cortex.
Auras (déjà vu, fear, rising epigastric, bad odors/tastes)[…] → behavioral arrest + vacant stare + impaired responsiveness + automatisms[…]. Lateralizing: ipsilateral hand automatisms + contralateral dystonic posturing.
Ictal speech localizes to nondominant[…] hemisphere; postictal nose wiping uses ipsilateral hand.
Treatment: relatively unlikely to respond to ASMs → epilepsy surgery[…]; seizure freedom in 90% after temporal lobectomy.